PANTIN 20 (Pantoprazole Gastro-Resistant Tablets 20 mg): Each Gastro resistant tablet contains Pantoprazole sodium sesquihydrate equivalent to Pantoprazole 20 mg.
PANTIN 40 (Pantoprazole Gastro-Resistant Tablets 40 mg): Each Gastro resistant tablet contains Pantoprazole sodium sesquihydrate equivalent to Pantoprazole 40 mg.
Pantoprazole is supplied as Gastro resistant tablet, available in two strengths (20 mg and 40 mg).
Each Pantoprazole Gastro resistant Tablet contains 45.11 mg or 22.55 mg of Pantoprazole sodium sesquihydrate (equivalent to 40 mg or 20 mg Pantoprazole, respectively).
Pantoprazole gastro-resistant tablet contains Pantoprazole, a proton pump inhibitors which inhibits the gastric H+K+ATPase which is responsible for acid secretion in the parietal cells of the stomach. Pantoprazole is white to off-white powder with a molecular weight of 432.4. Pantoprazole is freely soluble in water, very slightly soluble in phosphate buffer at pH 7.4, and practically insoluble in n-hexane. Pantoprazole is a racemic mixture with a melting point of 138°C. The chemical name for Pantoprazole is sodium-5-(difluoromethoxy)-2-[[(3,4-dimethoxy-2 pyridinyl)methyl] sulfinyl]-1 H-benzimidazole sesquihydrate.
Excipients/Inactive Ingredients: Lactose Monohydrate, Hydroxy Propyl Cellulose, Calcium Stearate, Sodium Carbonate Anhydrous, Sodium Lauryl Sulphate, Hypromellose, Ferric Oxide Yellow, Propylene Glycol, Titanium Dioxide, Methacrylic acid, Triethyl Citrate, Polysorbate 80 and Opecode Black S-1-17823.
Pharmacology: Pharmacodynamics: Pantoprazole is a substituted benzimidazole which inhibits the secretion of hydrochloric acid in the stomach by specific action on the proton pumps of the parietal cells. Pantoprazole is converted to its active form in the acidic canaliculi of the parietal cells where it inhibits the H+, K+-ATPase enzyme, i.e. the final stage in the production of hydrochloric acid in the stomach.
The inhibition is dose-dependent and affects both basal and stimulated acid secretion. In most patients, freedom from symptoms is achieved in 2 weeks. As with other proton pump inhibitors and H2 receptor inhibitors, treatment with pantoprazole causes a reduced acidity in the stomach and thereby an increase in gastrin in proportion to the reduce in acidity. The increase in gastrin is reversible.
Since pantoprazole binds to the enzyme distal to the cell receptor level, the substance can affect hydrochloric acid secretion independently of stimulation by other substances (acetylcholine, histamine, gastrin). The effect is the same whether the products is given orally or intravenously. The fasting gastrin values increase under pantoprazole. On short-term use, in most cases they do not exceed the normal upper limit. During long-term treatment, gastrin levels double in most cases. An excessive increase, however, occurs only in isolated cases. As a result, a mild to moderate increase in the number of specific endocrine (ECL) cells in the stomach is observed in a minority of cases during long-term treatment (simple to adenomatoid hyperplasia).
However, according to the studies conducted so far, the formation of carcinoid precursors (atypical hyperplasia) or gastric carcinoids as were found in animal experiments have not been observed in humans.
An influence of a long term treatment with pantoprazole exceeding one year cannot be completely ruled out on endocrine parameters of the thyroid and liver enzymes according to results in animal studies.
Pharmacokinetics: General pharmacokinetics: Pantoprazole is rapidly absorbed and the maximal plasma concentration is achieved even after one single 20 mg oral dose. On average at about 2.0 h-2.5 h p.a. the maximum serum concentrations of about 1-1.5 µg/ml are achieved, and these values remain constant after multiple administration. Volume of distribution is about 0.15 l/kg and clearance is about 0.1 l/h/kg.
Terminal half-life is about 1 h. There were a few cases of subjects with delayed elimination. Because of the specific binding of pantoprazole to the proton pumps of the parietal cell the elimination half-life does not correlate with the much longer duration of action (inhibition of acid secretion).
Pharmacokinetics do not vary after single or repeated administration. In the dose range of 10 to 80 mg, the plasma kinetics of pantoprazole are linear after both oral and intravenous administration.
Pantoprazole's serum protein binding is about 98%.
The substance is almost exclusively metabolized in the liver. Renal elimination represents the major route of excretion (about 80%) for the metabolites of pantoprazole, the rest is excreted with the faeces.
The main metabolite in both the serum and urine is desmethylpantoprazole which is conjugated with sulphate. The half-life of the main metabolite (about 1.5 h) is not much longer than that of pantoprazole.
Bioavailability: Pantoprazole is completely absorbed after oral administration. The absolute bioavailability from the tablet was found to be about 77%. Concomitant intake of food had no influence on AUC, maximum serum concentration and thus bioavailability. Only the variability of the lag-time will be increased by concomitant food intake.
Characteristics in patients/special groups of subjects: No dose reduction is requested when pantoprazole is administered to patients with restricted kidney function (incl. dialysis patients). As with healthy subjects, pantoprazole's half-life is short. Only very small amounts of pantoprazole can be dialyzed. Although the main metabolite has a moderately delayed half-life (2-3h), excretion is still rapid and thus accumulation does not occur.
Although for patients with liver cirrhosis (classes A and B according to Child) the half-life values increased to between 3 and 6 h and the AUC values increased by a factor of 3-5, the maximum serum concentration only increased slightly by a factor of 1.3 compared with healthy subjects.
A slight increase in AUC and Cmax in elderly volunteers compared with younger counterparts is also not clinically relevant.
Drug-Drug Interactions: Pantoprazole is metabolized mainly by CYP2C19 and to minor extents by CYPs 3A4, 2D6, and 2C9. In in vivo drug-drug interaction studies with CYP2C19 substrates (diazepam [also a CYP3A4 substrate] and phenytoin [also a CYP3A4 inducer)), nifedipine, midazolam, and clarithromycin (CYP3A4 substrates), metoprolol (a CYP2D6 substrate), diclofenac, naproxen and piroxicam (CYP2C9 substrates), and theophylline (a CYP1A2 substrate) in healthy subjects, the pharmacokinetics of pantoprazole were not significantly altered.
In vivo studies also suggest that pantoprazole does not significantly affect the kinetics of the following drugs (cisapride, theophylline, diazepam [and its active metabolite, desmethyldiazepam], phenytoin, warfarin, metoprolol, nifedipine, carbamazepine, midazolam, clarithromycin, naproxen, piroxicam, and oral contraceptives [levonorgestrel/ethinyl estradiol]). Dosage adjustment of these drugs is not necessary when they are coadministered with pantoprazole. In other in vivo studies, digoxin, ethanol, glyburide, antipyrine, caffeine, metronidazole, and amoxicillin had no clinically relevant interactions with pantoprazole.
Based on studies evaluating possible interactions of pantoprazole with other drugs, no dosage adjustment is needed with concomitant use of the following: theophylline, cisapride, antipyrine, caffeine, carbamazepine, diazepam (and its active metabolite, desmethyldiazepam), diclofenac, naproxen, piroxicam, digoxin, ethanol, glyburide, an oral contraceptive (levonorgestrel/ethinyl estradiol), metoprolol, nifedipine, phenytoin, warfarin, midazolam, clarithromycin, metronidazole, or amoxicillin.
There was also no interaction with concomitantly administered antacids.
There have been post marketing reports of increased INR and prothrombin time in patients receiving proton pump inhibitors, including Pantoprazole, and warfarin concomitantly [see Interactions].
Although no significant drug-drug interactions have been observed in clinical studies, the potential for significant drug-drug interactions with more than once-daily dosing with high doses of pantoprazole has not been studied in poor metabolizers or individuals who are hepatically impaired.
Other Effects: In a clinical pharmacology study, Pantoprazole 40 mg given once daily for 2 weeks had no effect on the levels of the following hormones: cortisol, testosterone, triiodothyronine (T3), thyroxine (T4), thyroid-stimulating hormone (TSH), thyronine-binding protein, parathyroid hormone, insulin, glucagon, renin, aldosterone, follicle-stimulating hormone, luteinizing hormone, prolactin, and growth hormone.
In a 1-year study of GERD patients treated with Pantoprazole 40 mg or 20 mg, there were no changes from baseline in overall levels of T3,T4, and TSH.
Pharmacogenomics: CYP2C19 displays a known genetic polymorphism due to its deficiency in some subpopulations (e.g., approximately 3% of Caucasians and African-Americans and 17% to 23% of Asians are poor metabolizers). Although these subpopulations of pantoprazole poor metabolizers have elimination half-life values of 3.5 to 10.0 hours in adults, they still have minimal accumulation (≤23%) with once-daily dosing. For adult patients who are CYP2C19 poor metabolizers, no dosage adjustment is needed.
Similar to adults, pediatric patients who have the poor metabolizer genotype of CYP2C19 (CYP2C19 *2/*2) exhibited greater than a 6-fold increase in AUC compared to pediatric extensive (CYP2C19 *1/*1) and intermediate (CYP2C19 *1/*x) metabolizers. Poor metabolizers exhibited approximately 10-fold lower apparent oral clearance compared to extensive metabolizers.
For known pediatric poor metabolizers, a dose reduction should be considered.
Animal Toxicology and/or Pharmacology: Studies in neonatal/juvenile and adult rats and dogs were performed. The data from these studies revealed that animals in both age groups respond to pantoprazole in a similar manner. Gastric alterations, including increased stomach weights, increased incidence of eosinophilic chief cells in adult and neonatal/juvenile rats, and atrophy of chief cells in adult rats and in neonatal/juvenile dogs, were observed in the fundic mucosa of stomachs in repeated-dose studies. Decreases in red cell mass parameters, increases in cholesterol and triglycerides, increased liver weight, enzyme induction, and hepatocellular hypertrophy were also seen in repeated-dose studies in rats and/or dogs. Full to partial recovery of these effects were noted in animals of both age groups following a recovery period.
Reproductive Toxicology Studies: Reproduction studies have been performed in rats at oral doses up to 450 mg/kg/day (88 times the recommended human dose based on body surface area) and rabbits at oral doses up to 40 mg/kg/day (16 times the recommended human dose based on body surface area) and have revealed no evidence of impaired fertility or harm to the fetus due to pantoprazole.
Pantoprazole Gastro-Resistant Tablets 20 mg: Mild reflux disease and associated symptoms (e.g. heartburn, acid regurgitation, pain on swallowing).
Long-term management and prevention of relapse in reflux oesophagitis.
Pantoprazole Gastro-Resistant Tablets 40 mg: Moderate and severe reflux oesophagitis.
Mild reflux disease and associated symptoms (e.g. heartburn, acid regurgitation, pain on swallowing): The recommended oral dosage is one gastro-resistant tablet Pantoprazole Gastro-Resistant Tablets 20 mg per day. Symptom relief is generally accomplished within 2-4 weeks, and a 4-week treatment period is usually required for healing of associated oesophagitis. If this is not sufficient, healing will normally be achieved within a further 4 weeks.
Long-term management and prevention of relapse in reflux oesophagitis: For long-term management, a maintenance dose of one gastroresistant tablet Pantoprazole Gastro-Resistant Tablets 20 mg per day is recommended, increasing to 40 mg pantoprazole per day if a relapse occurs.
Pantoprazole Gastro-Resistant Tablets 40 mg is available for this case. After healing of the relapse the dosage can be reduced again to 20 mg pantoprazole.
Treatment of Moderate and severe reflux oesophagitis: For the treatment of reflux esophagitis one tablet of Pantoprazole Gastro-Resistant Tablets 40 mg per day. In individual cases the dose may be doubled (increase to 2 tablets Pantoprazole Gastro-Resistant Tablets 40 mg daily) especially when there has been no response to other treatment.
Special Populations: Hepatic Impairment: A daily dose of pantoprazole 20 mg should not be exceeded in patients with severe liver impairment.
In patients with severe liver impairment the dose has to be reduced to 1 tablet (40 mg pantoprazole) every other day. Furthermore, in these patients the liver enzymes should be monitored during Pantoprazole Gastro-Resistant Tablets 40 mg therapy. In the case of a rise of the liver enzymes, Pantoprazole Gastro-Resistant Tablets 40 mg should be discontinued.
Renal Impairment: No dose adjustment is necessary in elderly patients of in those with impaired renal function.
Elderly: The daily dose of 40 mg pantoprazole should not be exceeded in elderly patients or in patients with impaired kidney function.
General instructions: Pantoprazole Gastro-Resistant Tablets tablets should not be chewed or crushed, and should be swallowed whole with water 1 hour before a meal.
A 4-week period is usually required for the treatment of reflux esophagitis. If this is not sufficient, healing will usually be achieved within a further 4 weeks.
There are no known symptoms of overdosage in man. In the case of overdosage with clinical signs of intoxication, the usual rules of intoxication therapy apply.
Pantoprazole gastro-resistent tablets must not be used in cases of known hypersensitivity to the active ingredient or/and any of the other constituents of Pantoprazole gastro-resistant tablets.
Pantoprazole, like other PPIs, should not be co-administered with atazanavir (see Interactions).
Hepatic Impairment: In patients with severe liver impairment the liver enzymes should be monitored regularly during treatment with pantoprazole, particularly on long-term use. In the case of a rise of the liver enzymes, the treatment should be discontinued (see Dosage & Administration).
Combination therapy: In the case of combination therapy, the prescribing information for the respective drugs must be observed.
Co-administration with NSAIDs: The use of pantoprazole gastro-resistant tablets 20 mg as a preventive of gastroduodenal ulcers induced by non-selective nonsteroidal anti-inflammatory drugs (NSAIDs) should be restricted to patients who require continued NSAID treatment and have an increased risk to develop gastrointestinal complications. The increased risk should be assessed according to individual risk factors, e.g. high age (>65 years), history of gastric or duodenal ulcer or upper gastro-intestinal bleeding.
In presence of alarm symptoms: In the presence of any alarm symptom (e.g. significant unintentional weight loss, recurrent vomiting, dysphagia, haematemesis, anaemia or melaena) and when gastric ulcer is suspected or present, malignancy should be excluded, as treatment with pantoprazole may alleviate symptoms and delay diagnosis. Further investigation is to be considered if symptoms persist despite adequate treatment.
Influence on vitamin B12 absorption: Pantoprazole, as all acid-blocking medicines, may reduce the absorption of vitamin B12 (cyanocobalamin) due to hypo- or achlorhydria. This should be considered in patients with reduced body stores or risk factors for reduced vitamin B12 absorption on long-term therapy or if respective clinical symptoms are observed.
Long term treatment: In long-term treatment, especially when exceeding a treatment period of 1 year, patients should be kept under regular surveillance.
Gastrointestinal infections caused by bacteria: Pantoprazole, like all proton pump inhibitors (PPIs), might be expected to increase the counts of bacteria normally present in the upper gastrointestinal tract. Treatment with pantoprazole gastro-resistant tablets may lead to a slightly increased risk of gastrointestinal infections caused by bacteria such as Salmonella and Campylobacter, and in hospitalized patients, possibly also Clostridium difficile.
Clostridium difficile-associated diarrhoea (CDAD) has been reported with use of nearly all antibacterial agents. For more information specific to antibacterial agents (clarithromycin and amoxicillin) indicated for use in combination with pantoprazole gastro-resistant tablets, refer to Warnings and Precautions sections of those package inserts.
Hypomagnesaemia: Severe hypomagnesaemia, symptomatic and asymptomatic, has been reported in patients treated with PPIs for at least three months, in most cases after a year of therapy. Serious manifestations of hypomagnesamia such as fatigue, tetany, delirium, convulsions, dizziness and ventricular arrhythmias can occur but they may begin insidiously and be overlooked. In most patients, treatment of hypomagnesemia required magnesium replacement and discontinuation of the PPI.
For patients expected to be on prolonged treatment or who take PPIs with medications such as digoxin or drugs that may cause hypomagnesaemia (e.g., diuretics), health care professionals may consider monitoring magnesium levels prior to initiation of PPI treatment and periodically. (See Adverse Reactions).
Bone Fractures: Several published observational studies suggest that proton pump inhibitor (PPI) therapy may be associated with an increased risk for osteoporosis-related fractures of the hip, wrist, or spine. The risk of fracture was increased in patients who received high-dose, defined as multiple daily doses, and long term PPI therapy (a year or longer). Patients should use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated. Patients at risk for osteoporosis related fractures should be managed according to established treatment guidelines (see Dosage & Administration and Adverse Reactions).
Concomitant use with Methotrexate: Literature suggests that concomitant use of PPIs with methotrexate (primarily at high dose; see methotrexate prescribing information) may elevate and prolong serum levels of methotrexate and/or its metabolite, possibly leading to methotrexate toxicities. In high-dose methotrexate administration a temporary withdrawal of the PPI may be considered in some patients (see Interactions).
Note: Prior to treatment a malignant disease of the esophagus or stomach should be excluded as the treatment with pantoprazole may alleviate the symptoms of malignant diseases and can thus delay diagnosis. Patients who do not respond after 4 weeks should be investigated. To date there has been no experience with treatment in children.
Risk of CLE and SLE: Cutaneous lupus erythematosus (CLE) and systemic lupus erythematosus (SLE) have been reported in patients taking PPIs. These events have occurred as both new onset and an exacerbation of existing autoimmune disease. The majority of PPI-induced lupus erythematosus cases were CLE.
The most common form of CLE reported in patients treated with PPIs was subacute CLE (SCLE) and occurred within weeks to years after continuous drug therapy in patients ranging from infants to the elderly.
Generally, histological findings were observed without organ involvement.
Systemic lupus erythematosus (SLE) is less commonly reported than CLE in patients receiving PPIs. PPI associated SLE is usually milder than non-drug induced SLE. Onset of SLE typically occurred within days to years after initiating treatment primarily in patients ranging from young adults to the elderly. The majority of patients presented with rash; however, arthralgia and cytopenia were also reported.
Avoid administration of PPIs for longer than medically indicated. If signs or symptoms consistent with CLE or SLE are noted in patients receiving Pantoprazole Gastro-Resistant Tablets, discontinue the drug and refer the patient to the appropriate specialist for evaluation. Most patients improve with discontinuation of the PPI alone in 4 to 12 weeks. Serological testing (e.g., Antinuclear antibody) may be positive and elevated serological test results may take longer to resolve than clinical manifestations.
Effects on the ability to drive and use of machines: Adverse drug reactions, such as dizziness and visual disturbances may occur (see Adverse Reactions). If affected, patients should not drive or operate machines.
Use in pregnancy: There are no adequate data from the use of pantoprazole in pregnant women. Studies in animals have shown reproductive toxicity. The potential risk for humans is unknown. Pantoprazole gastro-resistant tablets should not be used during pregnancy, unless clearly necessary.
Use in lactation: Animal studies have shown excretion of pantoprazole in breast milk. Excretion into human milk has been reported. Therefore, a decision on whether to continue/discontinue breast feeding or to continue/discontinue therapy with pantoprazole gastro-resistant tablets should be made taking into account the benefit of breastfeeding to the child, and the benefit of pantoprazole gastro-resistant tablets therapy to women.
Pregnancy: There are no adequate data from the use of pantoprazole in pregnant women. Studies in animals have shown reproductive toxicity. The potential risk for humans is unknown. Pantoprazole gastro-resistant tablets should not be used during pregnancy, unless clearly necessary.
Lactation: Animal studies have shown excretion of pantoprazole in breast milk. Excretion into human milk has been reported. Therefore, a decision on whether to continue/discontinue breast feeding or to continue/discontinue therapy with pantoprazole gastro-resistant tablets should be made taking into account the benefit of breastfeeding to the child, and the benefit of pantoprazole gastro-resistant tablets therapy to women.
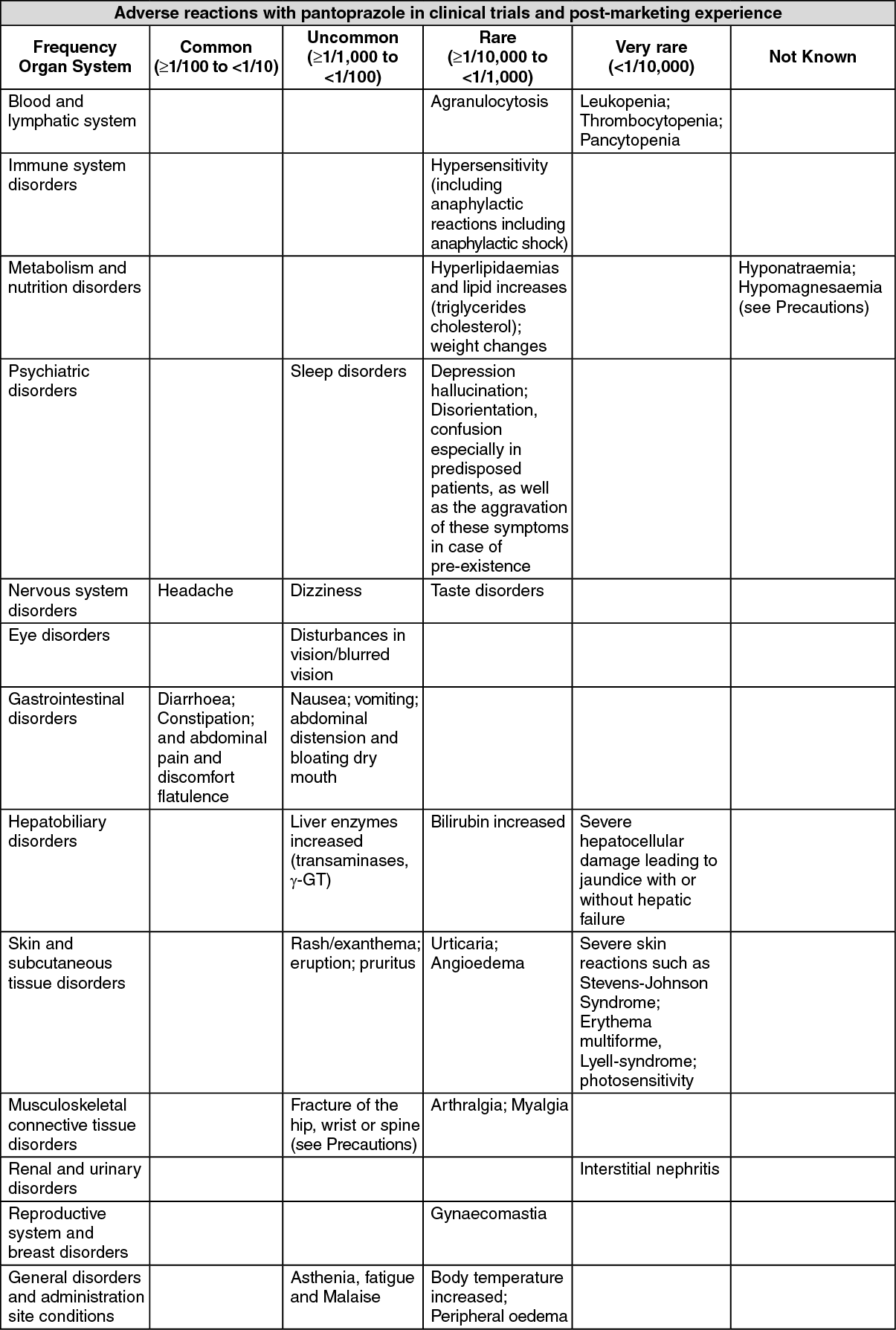
The adverse reaction profiles for Pantoprazole Gastro resistant Tablets are similar.
Approximately 5% of patients can be expected to experience adverse drug reactions (ADRs). The most commonly reported ADRs are diarrhoea and headache, both occurring in approximately 1% of patients.
The table as follows lists adverse reactions reported with pantoprazole, ranked under the following frequency classification: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from the available data).
For all adverse reactions reported from post-marketing experience, it is not possible to apply any Adverse Reaction frequency and therefore they are mentioned with a "not known" frequency. Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. (See table.)
 Click on icon to see table/diagram/image
Immune system:
Click on icon to see table/diagram/image
Immune system: systemic lupus erythematosus.
Skin and subcutaneous tissue: cutaneous lupus erythematosus.
Pantoprazole gastro-resistant tablets may reduce or increase the absorption of drugs whose bioavailability is pH-dependent (e.g. ketoconazole).
HIV medications (atazanavir): It has been shown that co-administration of atazanavir 300 mg/ritonavir 100 mg with omeprazole (40 mg once daily) or atazanavir 400 mg with lansoprazole (60 mg single dose) to healthy volunteers resulted in a substantial reduction in the bioavailibility of atazanavir. The absorption of atazanavir is Ph dependent. Therefore PPIs, including pantoprazole, should not be co-administered with atazanavir (see Contraindications).
Coumarin anticoagulants (phenprocoumon or warfarin): Although no interaction during concomitant administration of phenprocoumon or warfarin has been observed in clinical pharmacokinetic studies, a few isolated cases of changes in International Normalised Ratio (INR) have been reported during concomitant treatment in the post-marketing period. Therefore, in patients treated with coumarin anticoagulants (e.g. phenprocoumon or warfarin), monitoring of prothrombin time/INR is recommended after initiation, termination or during irregular use of pantoprazole.
Methotrexate: Case reports, published population pharmacokinefic studies, and retrospective analyses suggest that concomitant administration of PPIs and methotrexate (primarily at high dose) may elevate and prolong serum levels of methotrexate and/or its metabolite hydroxymethotrexate. However, no formal drug interaction studies of methotrexate with PPIs have been conducted (see Precautions).
Other interactions studies: Pantoprazole is metabolized in the liver via the cytochrome P450 enzyme system. The main metabolic pathway is demethylation by CYP2C19 and other metabolic pathways include oxidation by CYP3A4.
An interaction of pantoprazole with other drugs or compounds which are metabolized using the same enzyme system cannot be excluded. However, no clinically significant interactions were observed in specific tests with a number of such drugs or compounds, namely carbamazepine, caffeine, diazepam, diclofenac, digoxin, ethanol, glibenclamide, metoprolol, naproxen, nifedipine, phenytoin, piroxicam, theophylline and an oral contraceptive. Interaction studies with drugs also metabolized with these pathways, like carbamazepine, diazepam, glibenclamide, nifedipine, and an oral contraceptive containing levonorgestrel and ethinyl oestradiol, did not reveal clinically significant interactions.
Results from a range of studies demonstrate that pantoprazole does not effect the metabolism of active substances metabolised by CYP1A2 (such as caffeine, theophylline), CYP2C9 (such as piroxicam, diclofenac, naproxen), CYP2D6 (such as metoprolol), CYP2E1 (such as ethanol), or does not interfere with p-glycoprotein related absorption of digoxin.
There were also no interactions with concomitantly administered antacids.
Interaction studies have also been performed by concomitantly administering pantoprazole with the respective antibiotics (clarithromycin, metronidazole, amoxicillin). No clinically relevant interactions were found.
Store at or below 30°C and protect from moisture.
A02BC02 - pantoprazole ; Belongs to the class of proton pump inhibitors. Used in the treatment of peptic ulcer and gastro-oesophageal reflux disease (GERD).
Pantin 20/40 gastro-resistant tab 20 mg
30's
Pantin 20/40 gastro-resistant tab 40 mg
30's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
